This node has well-defined borders. Although the node displaces the SCM and the fat plane between node and muscle is not seen, there is no abnormal enhancement within the muscle itself. The visible fat planes show no signs of invasion.
The presence of non-enhancing (cystic or necrotic) regions within the node does not affect the assessment of iENE.
Grade 0
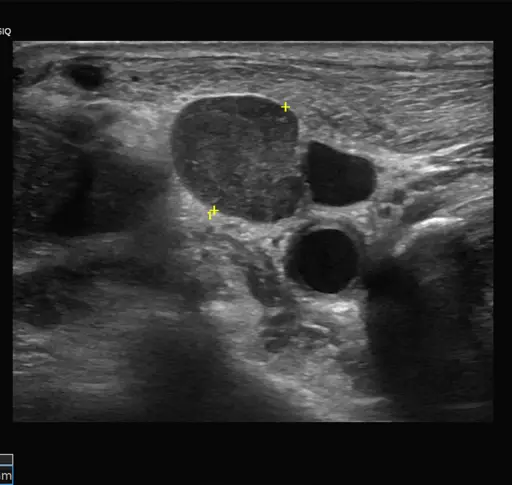
The heterogeneity and size of this node indicate malignancy, but it retains its well-defined borders. There is no indication that the heterogeneity represents matting of two nodes (one cystic and one solid) because mixed cystic-and-solid nodes are commonly seen in squamous cell carcinoma.
Grade 0
The node is slightly lobular, but the margins are sharply demarcated. Although his degree of lobulation might be seen with two matted nodes, it can also be seen as lobulation of a single pathologic lymph node. Therefore, this lobulation is not sufficient to indicate Grade 2 iENE. It is important to assess the node in multiple planes to determine whether it is a single lobular node or a cluster of matted nodes.
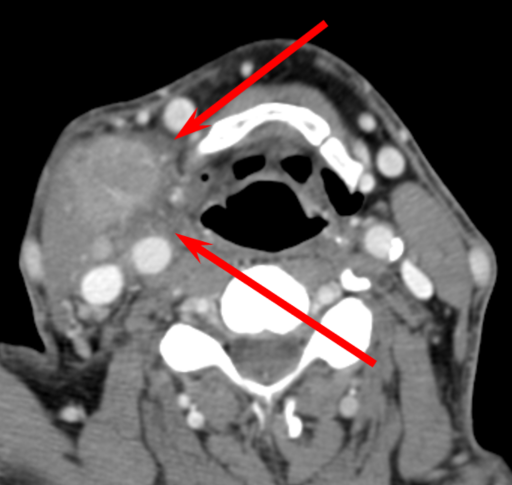
The arrows indicate areas of fat invasion along the medial aspect of the node. Usually, fat invasion is asymmetric or regional, as in this case, but it may occasionally be concentric.
You might be tempted to upgrade this node to Grade 3 because the fat plane adjacent to the SCM is invaded, and there may be a small area of invasion into muscle. But the findings in the muscle are not definitive, so they are not used to establish Grade of iENE.
Grade 1
The borders of this node show projections or spikes of enhancement extending into the surrounding fat, but not into the overlying muscle. These projections represent greater extranodal extent than an indistinct or irregular capsule (as might be seen in a normal node after irradiation), so this example is definitive for Grade 1 iENE.
Grade 1
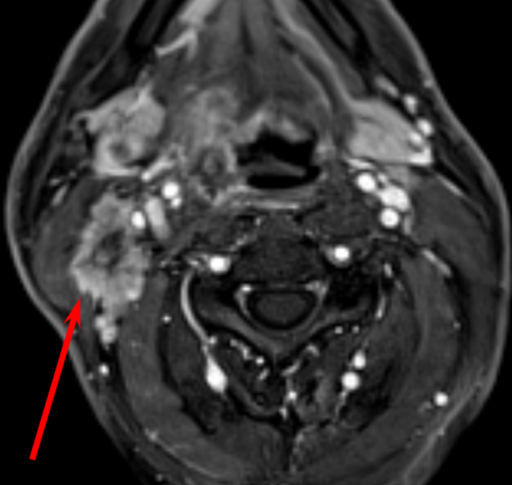
The margins of this node are not well-defined and there are projections or spikes of tumor (arrows) into the surrounding fat planes. Thus, this example is definitive for Grade 1 iENE.
The two submandibular nodes have merged into a single structure. You must definitively establish the involvement of multiple nodes in a cluster to distinguish a single lobulated node from a coalescent cluster of nodes. Multiple images, in multiple planes, are usually necessary.
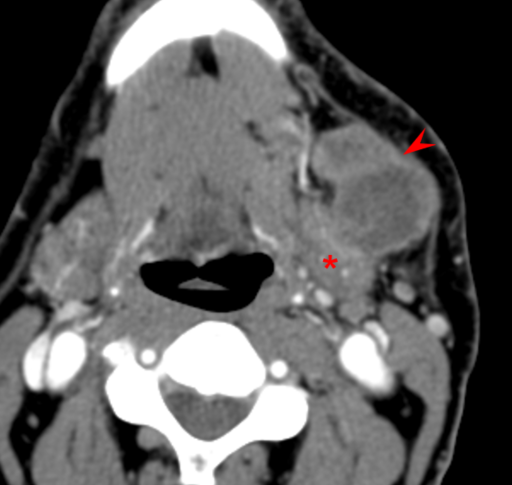
To establish Grade 2 iENE, three imaging criteria must be met on at least some of the images: 1) loss of fat planes between the nodes; 2) loss of convexity of at least one node at the point of contact; 3) loss of acute angle between nodes on at least one border (arrowhead).
This patient’s left submandibular gland (*) might be invaded, but more definitive evidence would be needed for this to be considered Grade 3 iENE for the purposes of staging.
Grade 2
In the first image, discrete nodes are visible, but on the second image (more anterior), the nodes have coalesced into a single mass with no visible boundary between them. Although early literature on iENE suggested that at least three nodes were need for a cluster to be considered “matted”, the current consensus is that two nodes are sufficient.
Skin involvement in this case is equivocal (even when viewed in all planes), not definitive, so Grade 3 should not be assigned.
Grade 2
There is unequivocal invasion into the perinodal fat (arrow), which would render this Grade 1 iENE. But there is also a defined plane (arrowheads) where two lymph nodes have coalesced. The three criteria for Grade 2 iENE are met: 1) loss of fat planes between the nodes; 2) loss of convexity of at least one node at the point of contact; 3) loss of acute angle between nodes on at least one border. Thus, this case should be upgraded to Grade 2 iENE.
Grade 2
The arrowheads indicate the plane at which the two nodes have coalesced, with:
loss of fat planes between the nodes
loss of convexity of at least one node at the point of contact
loss of acute angle between nodes on at least one border.
This is definitive coalescence of nodes, which indicates Grade 2 iENE. There is LIKELY invasion through the platysma muscle into the subcutaneous fat, but it is not definitive, so we cannot move up to Grade 3.
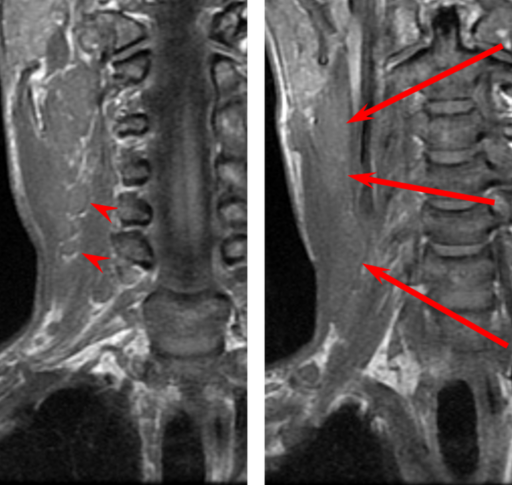
The SCM has been invaded by ENE from a lymph node in Level IIb. The portion of the muscle between the arrowheads is replaced by tumor. The muscle is not simply displaced or thinned; it has been replaced (invaded).
Grade 3
Most of the left SCM is no longer discernible. The tumor definitively extends through the platysma muscle and to the skin surface. Involvement of the neurovascular bundle is equivocal, and the IJV cannot be assessed on this unenhanced image, but there was already enough evidence to call this Grade 3.
Grade 3
The ill-defined nodal mass invades and destroys the SCM, and also invades into paraspinal muscles. Furthermore, the IJV has been obliterated. Invasion of the carotid artery is equivocal, but the muscular and venous invasion is already sufficient to call this Grade 3. This may be a coalescent mass of multiple nodes (which would indicate Grade 2), but the definitive Grade 3 findings render that discussion moot.
Grade 3
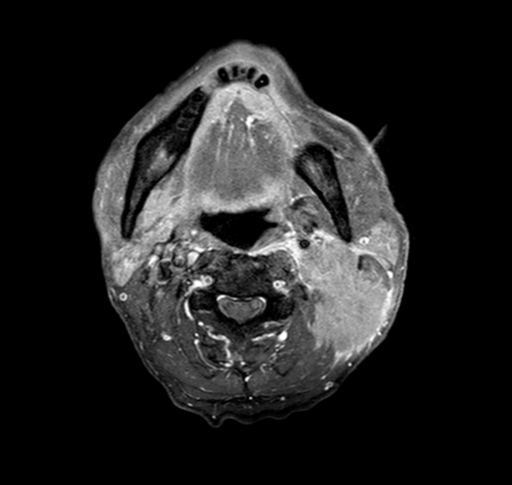
Tumor is seen between the internal carotid artery and external carotid branches (arrow). The internal jugular vein (arrowhead) is completely surrounded and invaded.
If all of the vessels had been displaced in the same direction, then this would not be definitive invasion. But when there is enhancing tumor between the vascular structures, it is definitive Grade 3 iENE.
Grade 3
Tumor fills the left carotid space. Even though the internal carotid artery is encased less than 270 degrees of its circumference (the nominal threshold for invasion), the involvement of the entire carotid space is sufficient to establish neurovascular invasion. When assessing patients for operability, other factors such as length of arterial involvement may be important, but these are not pertinent to the discussion of Grade 3 iENE.
Grade 3
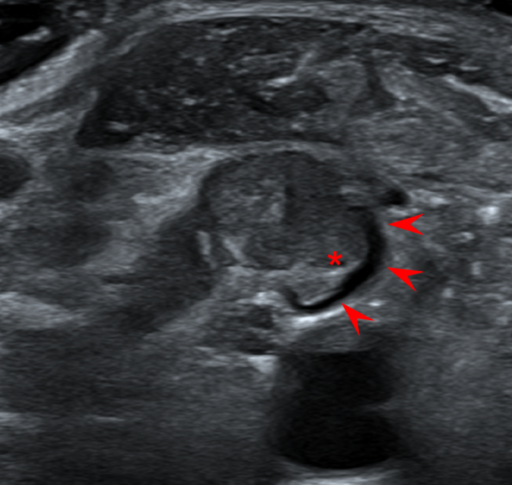
The metastatic node invades into the IJV (arrowheads), causing tumor thrombus (*). Only a thin rim of flowing blood (arrowheads) remains within the vein. To establish venous invasion, either tumor thrombus or complete occlusion is needed.
Note that contrast is not required for ultrasound assessment of venous invasion, but doppler (not shown) is useful to assess for residual flow.
Note that invasion of a minor vascular structure (like the anterior facial vein) is not adequate for establishing Grade 3 iENE. Major vascular structures are needed.
Grade 3
There are finger-like projections of tumor from the lymph node into the muscle body of the overlying SCM (arrow). The muscle is not simply displaced by tumor or draped over the tumor and thinned; tumor is visible within and between muscle bundles.