Round 3: Complex Cases and Borderline Cases
Grade 0
Grade 1
Grade 2
Grade 3



Grade 0
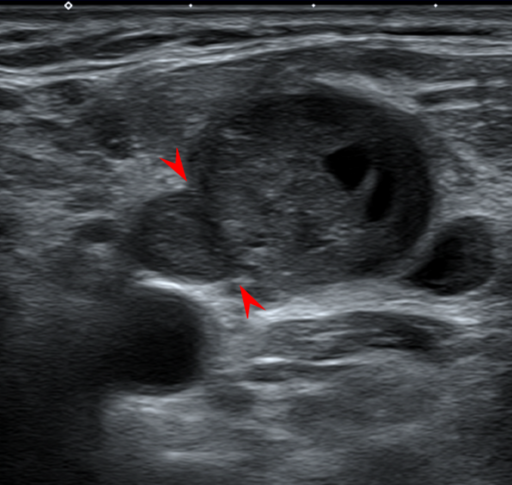
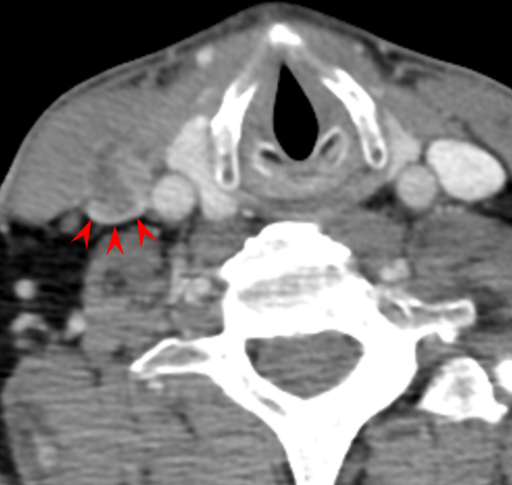
The fat planes between these nodes have been lost, but the acute angles at the edges of the contact planes are preserved (arrowheads). This is probable coalescence, but definitive coalescence is needed for establishing Grade 2 iENE. (The contralateral skin lesion is unrelated.)









Grade 3
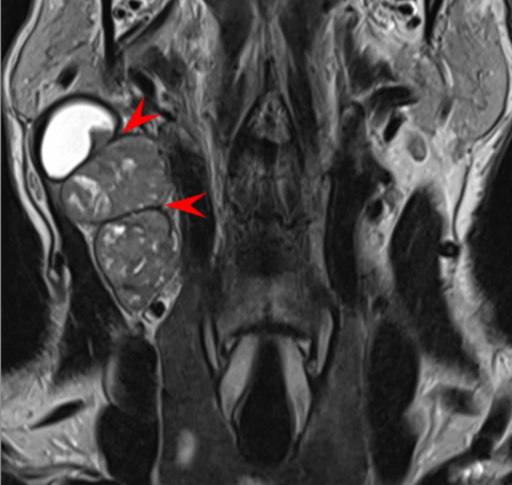
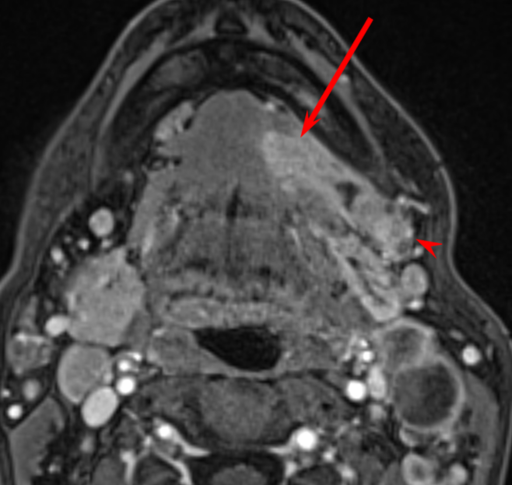
The T2-weighted image is not convincing because of the low-intensity rim around the lymph node that appears to separate it from the nearby soft tissues. But the post-contrast image shows definite invasion around the anterior aspect of the SCM, as well as the parotid gland. Remember to use all the sequences; don’t rely on just a single preferred sequence.
